Coping Styles and the Buffering Effects on Discrimination and Enacted Stigma in Transgender Individuals in the US
Kalei Glozier , Jae A. Puckett , Dee Jolly , Richard Mocarski , Debra A. Hope , L. Zachary DuBois
Transgender people experience minority stressors, enacted stigma, and discrimination, with negative implications for mental health. Although research is growing in this area, few studies have explored ways of coping with marginalization. In this sample of 158 transgender individuals, who were predominantly white (n = 109, 69%) and had a mean age of 33.06 (SD = 12.88), we used cluster analysis to identify patterns of coping and examined their potential buffering effects on the negative impacts of marginalization. Three coping clusters were identified: functional (n = 67; 43.2%), unhelpful (n = 23; 14.8%), and undifferentiated (n = 65; 41.9%). Approximately two-thirds of our sample experienced at least one instance of major discrimination in their lifetime, and our findings revealed that both enacted stigma and major discrimination were associated with lower satisfaction with life. The findings of this study suggest that at low to moderate levels of lifetime discrimination, participants in the functional or undifferentiated coping groups had higher levels of life satisfaction than participants in the unhelpful coping group. However, at high levels of lifetime discrimination, there was little difference in life satisfaction based on coping. In comparison, there was not a significant moderating effect for past-year enacted stigma.
- Volume (Issue)
- 4(4)
- Published
- December 15, 2025
- DOI
- 10.57814/d4x3-tc10
- Copyright
- © 2025. The Authors. This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License (CC BY-NC-ND 4.0)
- Preferred Citation
- Glozier, Kalei, Puckett, Jae A., Jolly, Dee, Mocarski, Richard, Hope, Debra A., DuBois, L. Zachary. 2025. "Coping Styles and the Buffering Effects on Discrimination and Enacted Stigma in Transgender Individuals in the US." Bulletin of Applied Transgender Studies 4 (4): 265-282. https://doi.org/10.57814/d4x3-tc10
Transgender people represent a broad group whose gender identities differ from that typically associated with their sex assigned at birth. This group includes trans men, trans women, genderqueer, and nonbinary people, among others (Tompkins 2021). Transgender people experience a variety of minority stressors, one of which is discrimination. Experiences of discrimination are embedded within power structures that privilege cisgender, white, heterosexual individuals, and people with other dominant identities. These power structures intersect across various identities and simultaneously shape exposure to marginalization (Collins 1990; Taylor 2017).
As mentioned, experiencing discrimination is one aspect of minority stress. Minority stress refers to the unique stressors that marginalized groups experience, above and beyond the general stressors that anyone may encounter (Brooks 1981; Meyer 2003). Meyer’s minority stress model for sexual minorities specifically identified distal stressors, meaning overt or enacted forms of minority stress like victimization and discrimination, and proximal stressors, which can be thought of as reactions to distal stressors. Proximal stressors included expectations of rejection, identity concealment, and internalized stigma. This model originated with a focus on cisgender lesbian, gay, and bisexual individuals (Brooks 1981; Meyer 2003) and was later adapted and refined to apply to transgender individuals (Hendricks and Testa 2012; Testa et al. 2015).
Research on enacted stigma, such as discrimination, rejection, and other distal or more overt acts of marginalization, has documented high rates of hardship for transgender people. In the US, up to 50% of transgender people report physical violence in their lifetime (Stotzer, 2009), 1 out of 10 report physical violence in the past year (James et al. 2016), and 1 out of 4 report discrimination in the past year (Puckett et al. 2019). In addition, the effects of enacted stigma are amplified when individuals hold multiple marginalized identities due to overlapping systems of power, including structural racism, heterosexism, and cissexism. For example, in the US, transgender people with lower socioeconomic status experience higher rates of sexual violence (Testa et al. 2012), transgender people of color (TPOC) experience higher levels of distress than white transgender people (Lefevor et al. 2019a), and Black transgender women experience deadly violence at much higher rates compared to other racial groups (Krell 2017).
Due to these experiences of minority stress, transgender people experience significant mental health disparities including higher rates of depression and anxiety symptoms relative to cisgender people (Lefevor et al. 2019b). Similarly, one study examining transgender participants in a nested matched-pair study with cisgender participants found that transgender participants were significantly more likely to endorse a lifetime suicide attempt and suicidal ideation (29% of the transgender sample) than cisgender participants (8.5% of the cisgender sample; Reisner et al. 2014). These findings are further supported by the 2015 US Trans Survey, which found that 39% of participants were currently experiencing psychological distress, which is drastically higher than the rate of 5% in the general US population (James et al. 2016).
Life satisfaction is an often-overlooked component of well-being and mental health in transgender populations and little research has examined this in relation to minority stress. Research shows that transgender individuals in a sample from Norway reported significantly lower levels of satisfaction with life than their cisgender peers (Anderssen et al. 2020). Given these lower overall levels of life satisfaction, more work is needed exploring potential drivers and correlates of life satisfaction for transgender people. In one sample of 92 transgender individuals, 48.4% of the sample reported they were satisfied with their lives and higher levels of life satisfaction were associated with older age, higher education, and favorable self-rated health (Grupp et al. 2023). Another study found that life satisfaction was positively associated with psychological functioning, satisfaction with social gender congruence, satisfaction with physical gender congruence, and quality of life (Jones et al. 2018). Research also shows, in cisgender samples, a reciprocal relationship with mental health, such that mental health challenges decrease one’s satisfaction with life, and lower life satisfaction is associated with an increased likelihood of psychiatric disorders (Fergusson et al. 2015). We aim to expand this research on life satisfaction by exploring associations with enacted stigma and coping profiles among transgender people in the US.
Considering the high rates of minority stress experienced by transgender people and the implications for mental health and life satisfaction, identifying useful coping strategies may help alleviate some distress in this marginalized community. Past research on coping in transgender samples has primarily explored individual coping strategies in isolation or in parallel rather than examining more holistic profiles of coping. For instance, Grossman et al. (2011) found that emotion-oriented coping predicted negative mental health outcomes in a sample of transgender youth. Similarly, Puckett et al. (2020) found that using unhelpful coping strategies of coping via detachment, substance use, and internalization were associated with higher levels of anxiety and depression. Research has also found that using social support to cope, a helpful coping strategy, was associated with lower reported depressive symptoms (Rotondi et al. 2011). While the literature detailing coping techniques of transgender people is growing, research has not, to our knowledge, examined the association between coping and life satisfaction in transgender individuals.
Although these past studies shed light on individual coping strategies, they do not provide a more holistic understanding of coping. Instead, research is needed that considers, simultaneously, the use of a variety of coping strategies, to more accurately represent how transgender people may be responding to stressors. There has been one study (Freese et al. 2018) to take such an approach with transgender people, which used cluster analyses to find distinct coping profiles. They found three coping profiles in their sample. One group had high functional and low dysfunctional coping (HFLD), which was characterized by primarily using coping strategies aligned with the positive self-efficacy and social support factors, while rarely engaging in strategies associated with the negative self-directed or substance use factors. The authors also found a group they described as having low functional and low dysfunctional coping (LFLD), which was characterized as a group who infrequently engaged in any of the designated coping strategies. The final group the authors found included participants who used high functional and high dysfunctional coping (HFHD), suggesting participants in this group were highly engaged in all coping strategies. The LFLD group and the HFHD group had significantly higher odds of reporting more severe levels of depression compared to participants in the HFLD group. The HFHD group had significantly higher odds of reporting suicidality before transitioning and affirming their gender than participants with the HFLD coping profile and higher odds of reporting suicidality during the beginning of their transition compared to participants with HFLD and LFLD coping profiles (Freese et al. 2018).
This past research demonstrates that examining coping at broader levels that considers various types of coping simultaneously can add more complex understandings about transgender people’s coping responses, with implications for understanding mental health and wellbeing. As highlighted by Freese et al. (2018), when individual coping strategies are studied in isolation, this may provide a skewed understanding of coping that is not reflective of the breadth of possible responses to stress. As there has been limited research examining coping in more holistic ways, we sought to add to the literature in this area.
Current Study
The focus of the current study was to understand the relationships between coping, experiences of discrimination and enacted stigma, and life satisfaction for transgender people. We also were interested in understanding coping in a more complex way that can simultaneously account for the various forms of coping that transgender people may engage in, rather than examining distinct forms of coping in isolation. As such, we explored patterns in coping profiles. In addition, we examined the potential moderating effect of coping profiles on the relationship between discrimination and enacted stigma with life satisfaction.
Method
This data was collected as part of a larger mixed-methods longitudinal study examining health and resilience among transgender people (N = 158) in relation to sociopolitical contexts. Participants were recruited via advertisements distributed to community organizations, social media, snowball sampling, and in-person events (e.g., Pride festivals). Data collection was conducted in four states (Oregon, Michigan, Tennessee, and Nebraska), selected given the range of sociopolitical climates represented in terms of support and protections for transgender people. Interested participants completed an online screener that included basic demographic information. The screener data was then used to maximize recruitment efforts to include a diverse sample regarding gender identity, racial identity, rural/urban residence, and age. To guard against fraudulent responders and bots, we utilized prevention mechanisms in Qualtrics (e.g., ballot stuffing prevention) and we reviewed screener responses for repeat participants, suspicious entries, and other information that could indicate attempts to infiltrate the study (e.g., indicating a cisgender identity although study was advertised for transgender people). At baseline, participants completed a set of questionnaires, an in-person interview, and the collection of several stress and health biomarkers (e.g., blood pressure, salivary stress hormones, and immune measures). This baseline data was collected between late September 2019 and early March 2020. Eligibility for the study was as follows: living in Oregon, Michigan, Nebraska, or Tennessee; ages 19 or over (the age of consent in Nebraska); and transgender identified. The University of Oregon Institutional Review Board approved the study. All participants provided their informed consent before participation. Participants were paid via an electronic gift card for each portion of the study they participated in, with the potential to earn up to $250.
Measures
Demographics
Participants completed demographic questions including age, gender identity (assessed with two items – one with an extensive set of response options and a second question where participants would select one of three categories; both asked participants to select the label that best represented their experiences), sex assigned at birth, state, income, and racial identity. See Table 1 for response options for these items.
Discrimination
Participants reported their experiences of discrimination by completing the Major Experiences of Discrimination Scale (Williams et al. 1997; Williams et al. 2008). This included 9 items, such as: “For unfair reasons, have you ever not been hired for a job?” If the participant indicated that they had the experience listed in each item, they were then asked, “What do you think was the main reason for this experience?” Participants were then able to select what they thought was the main reason for this discrimination, with the following options: ancestry or national origins, gender, race, age, religion, height, weight, some other aspect of your physical appearance, sexual orientation, and education or income level. Participants also indicated the last time each form of discrimination occurred, with the following response options: within the past week, the past month, the past year, or more than a year ago.
Enacted Stigma
The Gender Minority Stress and Resilience (GMSR) measure was used to assess experiences of enacted stigma via gender-related discrimination (e.g., “I have had difficulty finding housing or staying in housing because of my gender identity or expression”), gender-related rejection (e.g., “I have been rejected or distanced from friends because of my gender identity or expression”), and gender-related victimization (e.g., “I have been threatened with physical harm because of my gender identity or expression”) subscales (Testa et al. 2015). For each item, participants indicated if they had this experience in the past year, after the age of 18, before the age of 18, and never. For parsimony, we calculated a sum score across these subscales to reflect overall levels of enacted stigma in the past year (DuBois et al. 2024).
Coping
The Brief COPE included 28 items pertaining to how participants dealt with problems that occurred in their day-to-day lives, with 14 subscales measuring different coping styles (Carver 1997). Examples include “I’ve been turning to work or other activities to take my mind off things” and “I’ve been accepting the reality of the fact that it has happened.” Participants were asked to indicate how frequently they engaged in each type of coping on a scale from 1 (I haven’t been doing this at all) to 4 (I’ve been doing this a lot). Each subscale consisted of two items that were summed to give a score of how frequently each coping technique was used. This measure is intended to reflect a variety of helpful and unhelpful forms of coping.
Satisfaction with Life
The Satisfaction with Life Scale included five items measuring cognitive judgments of one’s satisfaction (Diener et al. 1985). For example, items included the following: “I’m happy with my life.” Participants rated how much they agreed or disagreed with each of the five items using a 7-point scale (1 = strongly disagree; 7 = strongly agree). Responses were summed to indicate participants’ overall satisfaction with life. In the current study, Cronbach’s alpha was .89.
Participants
There was a total of 158 participants across Oregon (n = 45; 28.5%), Michigan (n = 39; 24.7%), Nebraska (n = 35; 22.2%), and Tennessee (n = 39; 24.7%). Participants ranged in age from 19-70 years old (M = 33.06; SD = 12.88) and had a variety of gender identities: 27.2% identified as trans men/men, 26% identified as trans women/women, and the remaining participants identified with terms like genderqueer, nonbinary, and others described in Table 1. For racial identity, 5.1% (n = 8) of the sample identified as Black or African American, 1.3% (n = 2) identified as American Indian or Alaskan Native, 3.8% (n = 6) identified as Asian, 3.8% (n = 6) identified as Latinx, 69% (n = 109) identified as white, 16.5% (n = 26) identified as Multiracial/Multiethnic, and 0.6% (n = 1) reported that their identities were not listed. See Table 1 for additional demographic information.
Statistical Analyses
SPSS was used for all analyses. We began by calculating basic descriptive information about the sample and rates of experiencing discrimination and enacted stigma. We also examined correlations between discrimination, past-year enacted stigma, and life satisfaction. We were interested in forms of coping and how these may buffer the effects of discrimination and enacted stigma on satisfaction with life. To assess different coping profiles, we conducted a k-means cluster analysis. Unique groups of participants were identified based on their responses to the BRIEF Cope scale. We examined an increasing number of clusters and determined our final number of clusters by reviewing the qualities of the clusters and interpretability, as well as sample size. Each person was assigned to a specific cluster, and this information was used in subsequent analyses. An ANOVA was conducted to assess differences in life satisfaction across the clusters. Finally, we used the PROCESS macro (Hayes 2022) to conduct two moderation analyses to assess whether the coping clusters moderated the effects of discrimination and enacted stigma on life satisfaction.
Results
On average, participants endorsed approximately 2 (1.83) forms of discrimination on the Major Experiences of Discrimination Scale, with 35.9% reporting never experiencing any discrimination (see Table 2 for more details). More than 10% of the sample reported experiencing 4 or more forms of discrimination experiences in their lifetime. Over one-fourth (28.2%) of the sample reported that they had been unfairly fired, 29.5% of the sample reported that they had not been hired for a job for unfair reasons, 25.6% reported that they had been denied a promotion for unfair reasons, 27.6% reported having received worse service (such as from a plumber or mechanic), 18.6% reported being unfairly discouraged by a teacher or advisor from continuing their education, 17.9% reported ever moving into a neighborhood where neighbors made life difficult for them or their families, 9% reported being unfairly prevented from moving into a neighborhood because the landlord or a realtor refused to sell or rent them a house or apartment, and 1.3% reported they had been unfairly denied a bank loan. These experiences of discrimination were mostly related to gender identity and gender expression and presentation (see Table 3).
As expected, there was a correlation between experiencing enacted stigma in the past year with lifetime experiences of discrimination (r = .31, p < .001). Reporting more lifetime experiences of discrimination was associated with less life satisfaction (r = –.22, p < .01). In addition, reporting more experiences of enacted stigma in the past year was associated with less life satisfaction (r = –.30, p < .001).
In the cluster analysis, there were three groups. Cluster 1 (Functional Coping; n = 67; 43.2%) included participants who were more likely to use functional coping strategies such as active coping, use of support, venting, planning, and acceptance. Cluster 2 (Unhelpful Coping; n = 23; 14.8%) included participants who were more likely to use unhelpful coping strategies such as disengagement, denial, substance use to cope, distraction, and self-blame and a lower likelihood of using more helpful or functional strategies. Cluster 3 (Undifferentiated Coping; n = 65; 41.9%) included participants who had lower scores than average on the coping subscales overall but tended to use the various types of coping to similar degrees, with no singular coping characteristic defining this group.
The demographics of the clusters were largely similar including in relation to gender, sex assigned at birth, rural/urban location, state, income, and race. Cluster 2 (M = 27.35, SD = 10.39) was significantly younger than Cluster 3 (M = 35.83, SD = 14.77); F (2, 152) = 4.23, p < .05. There were no significant differences in age between Cluster 1 and 2 or between Cluster 1 and 3. Overall, there was a significant difference between the groups on life satisfaction scores; F (2, 151) = 11.29, p < .001. Clusters 1 (Functional Coping; M = 19.44, SD = 7.30) and 3 (Undifferentiated Coping, M = 20.55, SD = 7.68) had higher levels of life satisfaction than Cluster 2 (Unhelpful Coping, M = 12.21, SD = 6.56).
In the first moderation analysis, we examined whether there was an interaction between coping profiles (Cluster 2, Unhelpful Coping, as the reference group) and lifetime discrimination in relation to life satisfaction, while controlling for age (see Table 4). The coping profiles and lifetime discrimination explained 23.75% of the variance in life satisfaction. The addition of the interaction terms accounted for 4.2% of the variance in life satisfaction.
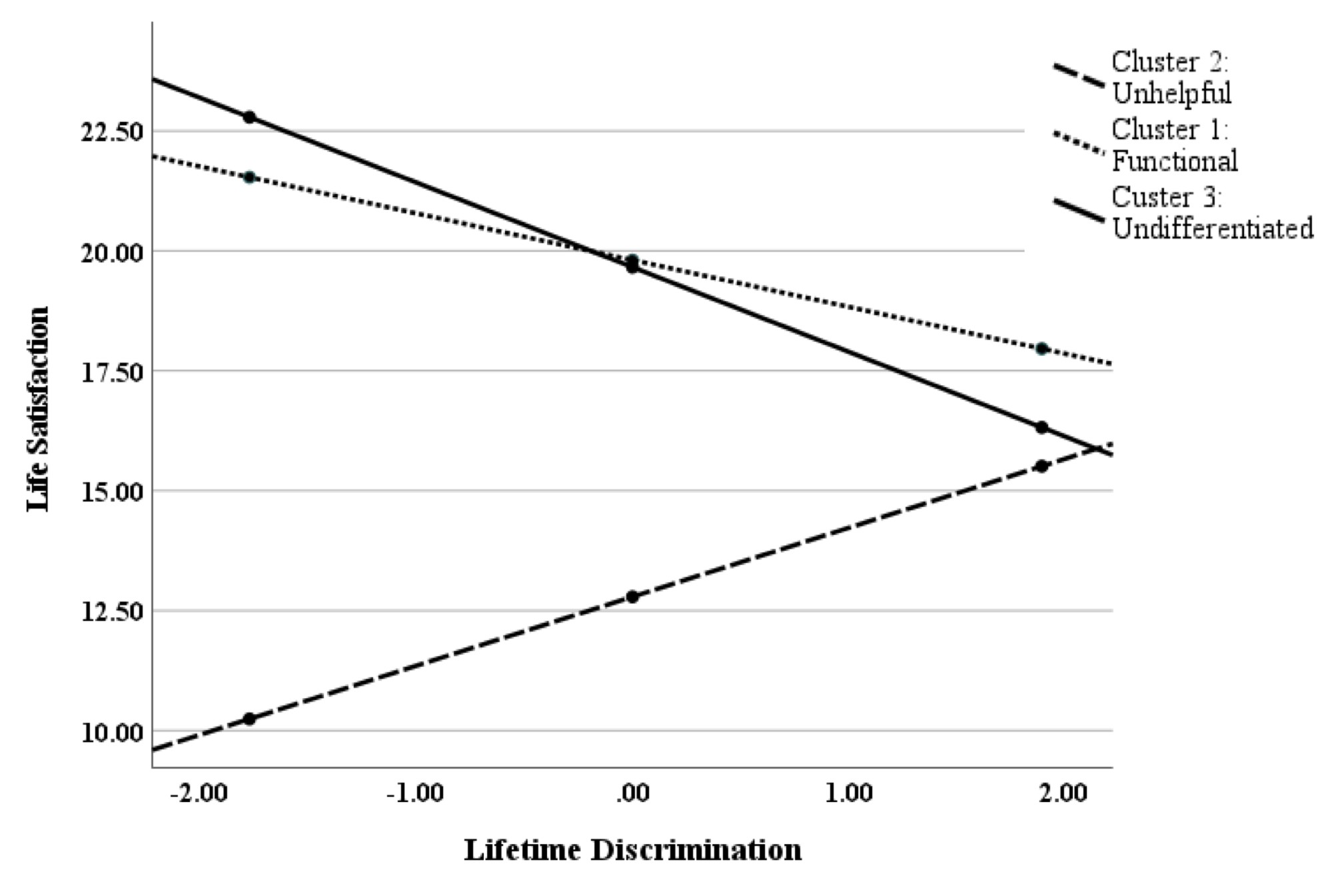
Figure 1 portrays the associations between lifetime discrimination and life satisfaction for each of the clusters. At low and average levels of lifetime discrimination, Cluster 1 (Functional Coping) and Cluster 3 (Undifferentiated Coping) had higher levels of life satisfaction compared to participants in Cluster 2 (Unhelpful Coping). However, the magnitude of these differences decreased as levels of lifetime discrimination increased. Cluster 1 (Functional Coping) and Cluster 3 (Undifferentiated Coping) saw decreasing levels of life satisfaction as levels of enacted stigma increased. As a result, at higher levels of lifetime discrimination, there were not significant differences in life satisfaction across the three groups. There was a significant negative association between lifetime discrimination and life satisfaction for Cluster 1 (Functional Coping; b = –2.41, SE = 1.11, t = –2.16, p < .05) and Cluster 3 (Undifferentiated Coping; b = –3.20, SE = 1.13, t = –2.82, p < .01).
In the second moderation analysis, we examined whether there was an interaction between coping profiles (Cluster 2, Unhelpful Coping, as the reference group) and past-year enacted stigma in relation to life satisfaction, while controlling for age. The coping profiles and past-year enacted stigma explained 19.82% of the variance in life satisfaction. Participants who used typically defined “healthy” coping mechanisms, Cluster 1, and participants in Cluster 3, with undifferentiated approaches to coping, had higher levels of life satisfaction than participants in Cluster 2 (Unhelpful Coping), however, the moderation findings were not significant (see Table 5).
Discussion
Approximately two-thirds of our sample experienced at least one instance of major discrimination in their lifetime. These rates of discrimination are higher than what has been reported in many other studies (e.g., Handal et al. 2023; Whitaker et al. 2017; Zilioli et al. 2023), although some studies have reported a similar or higher rate of major discrimination experiences over the lifetime (Braksmajer et al. 2018; Cenat et al. 2022). Importantly, these studies were conducted with communities with different sociodemographic characteristics from the participants of our study. Much of the previous research has been focused on understanding the experiences of major discrimination in different racial and ethnic communities (Cenat et al. 2022; Handal et al. 2023; Whitaker et al. 2017; Zilioli et al. 2023), with our study contributing to assessing various types of discrimination in a transgender sample.
We originally intended to study intersectional forms of discrimination, however, due to the limited sample size and low endorsement of discrimination attributed to holding other identities, we were not able to explore this area further. Discrimination research often focuses on a single aspect of identity and relies predominantly on white samples (Vargas et al. 2020), leaving unanswered questions about the experiences of transgender individuals who hold multiple marginalized identities. The Major Experiences of Discrimination Scale (Williams et al. 1997; Williams et al. 2008) was used to determine what aspects of identity participants considered the reason for discrimination they experienced, however, this required participants to select a single identity they mainly attributed this to. With this sample, most participants indicated their experiences of discrimination were tied to their gender identity and presentation, with little endorsement of discrimination in other areas. For participants with marginalized racial identities in our sample, it may have been difficult to separate aspects of their identity when indicating why an experience of discrimination happened, such as questioning whether a person was denied a job because of their gender or their race. This highlights that scales like these often make measuring intersectionality challenging. Other research has discussed this challenge, highlighting a need for a more comprehensive understanding of intersectional experiences of discrimination (Bowleg 2013; Cuádraz and Uttal 1999). Future research might benefit from using other measures, such as the LGBTQ+ People of Color Microaggressions Scale (Huynh et al. 2024) or the Intersectional Discrimination Index (Scheim and Bauer 2019).
Aligned with other literature (Chan et al. 2021; Conlin et al. 2017; Janssen et al. 2023), we found that both enacted stigma and major discrimination were associated with lower levels of satisfaction with life. Our findings extend the findings of previous research by highlighting this relationship among a sample of transgender people. Life satisfaction is known to be lower among transgender people than among cisgender people (Anderssen et al. 2020) and our results suggest that this difference may be related to anti-transgender discrimination and enacted stigma. The importance of these findings is underscored by past research showing that life satisfaction is associated with overall physical, psychological, and behavioral health (Hughto et al. 2015; Kim et al. 2021; Lawrence et al. 2022). Our results suggest that life satisfaction may represent an important pathway through which enacted stigma and discrimination become embodied to affect health among transgender people, although the relationship with health was not directly tested in the present analyses.
In relation to coping, it was encouraging to see that most of our sample endorsed either functional or undifferentiated coping profiles and that only a minority, 14.8%, were classified into the unhelpful coping patterns group. In the face of pervasive hardships and minority stress, finding effective ways of coping can be a challenge. Even so, most of our participants were coping in ways that appeared to be beneficial to their mental health and well-being.
The clusters that we obtained in our analysis differ somewhat from the findings by Freese et al. (2018), who found three groups based on coping profiles: high functional/low dysfunctional, high functional/high dysfunctional, and low functional/low dysfunctional. In their study, they found that transgender people in the high functional/high dysfunctional coping group had worse outcomes, particularly in relation to suicidality. It is possible that this group of transgender people are encountering high levels of minority stress and therefore coping is somewhat dysregulated and unpredictable, or that there may be other contextual factors that interfere with the effectiveness of the coping strategies used. In our work, we found a group that had lower scores than average on the coping subscales overall but tended to use the various types of coping to similar degrees, with no singular coping characteristic defining this group. This cluster was comparable to the group that endorsed more use of the functional coping strategies in relation to their life satisfaction and the moderating effects on lifetime discrimination. It is possible that our findings differ from Freese et al. due to the magnitude of use of the unhelpful coping strategies. It can sometimes be helpful to engage in coping that might be self-protective yet traditionally grouped as an unhelpful coping strategy, such as when avoiding dangerous situations. Yet, when unhelpful coping strategies are heavily relied upon, it could be detrimental to one’s wellbeing. Given this possibility, we believe that the undifferentiated coping group in our findings may reflect a more flexible approach to coping that could be responsive to contextual demands.
Our findings indicate that, at low to moderate levels of lifetime discrimination, participants in the functional coping and undifferentiated coping groups had higher levels of life satisfaction compared to participants in unhelpful coping group. At high levels of lifetime discrimination, the buffering effect had lessened, and there were no meaningful differences between the groups. This seems to indicate that coping strategies, as assessed via our general measure of coping, can foster positive adaptation in the face of lifetime discrimination, but that this may be more challenging as the exposure to minority stress increases. For people who are experiencing regular occurrences of discrimination, the effectiveness of coping strategies may diminish. Furthermore, there was not a significant buffering effect in the analysis on past-year enacted stigma. As such, there did not appear to be a protective effect in relation to more recent experiences of minority stress. Our study findings highlight the importance of change at the structural level to decrease exposure to enacted stigma. Placing the burden on transgender people to cope with marginalization can reinforce power hierarchies and addressing the root causes of marginalization is needed to support better mental health outcomes as well.
Limitations
There are several limitations to these analyses. First, though this sample is adequate for such an in-depth mixed-methods study centering transgender people, this is a relatively small sample of transgender people in the US as a whole and larger samples are needed in this area of study. We nearly reached our goal of 50% TPOC in the Michigan and Oregon subsamples, however, despite our efforts to reach a more diverse sample, we were unable to recruit a racially diverse subsample in Nebraska and Tennessee. Due to the limited amount of racial diversity, our ability to determine how these relationships differed between TPOC and white transgender people was restricted. Many factors could have impacted our ability to connect with TPOC, including potential participants not feeling represented or not having trust in the research team given the racial identities of the primary researchers, the lack of trust for the university systems, and the access barriers faced by many communities of color that impact the ability to participate in research. Furthermore, the cross-sectional nature of these data makes it impossible to determine the causal nature of these relationships. Longitudinal research is needed to determine how discrimination, enacted stigma, and coping affect life satisfaction over time and how coping may influence these trajectories.
In this study, we measured coping using a general measure of coping which means that other transgender specific ways of coping may be overlooked. Past research shows that transgender people may enact identity specific forms of coping (Owens et al. 2023), such as engaging in self-affirming behaviors (Sherman et al. 2021). More recent measure development research has expanded the possibilities for assessing coping in transgender communities in future research (Lindley and Budge 2024). It also is critical that future research examine more liberatory approaches as overly focusing on coping may inadvertently reinforce power hierarchies (Phillips et al. 2015). Integrating concepts like critical consciousness, empowerment, and collective action may help to push beyond the individual and their responsibility to cope with oppression.
Implications
Understanding the coping patterns of transgender individuals is critical for providing effective support in the mental health field. Coping mechanisms employed by transgender individuals in response to societal stigma and discrimination can significantly impact their mental health and well-being (Budge et al. 2013; Lindley and Budge 2024). By gaining insight into how transgender people cope effectively in the face of minority stress, we can tailor support to the unique needs of transgender individuals and ultimately better promote resilience and empowerment. Additionally, understanding coping strategies allows for the development of interventions aimed at reducing minority stressors and improving mental health outcomes and life satisfaction within transgender communities (Anderssen et al. 2020; Chan et al. 2021; Conlin et al. 2017; Hughto et al. 2015; Janssen et al. 2023).
Conclusion
Overall, we found relationships between lifetime experiences of discrimination, past year anti-transgender enacted stigma, and satisfaction with life. We also found there are distinct coping groups that can be meaningfully delineated and that these patterns of coping impact the effect of discrimination on satisfaction with life. We found that participants who endorsed functional and flexible or undifferentiated coping styles experienced less of an effect from lifetime discrimination on life satisfaction, particularly at low to moderate levels of discrimination. These results challenge previous views of coping which view coping strategies independently and highlight the need to view responses to stressors through a more holistic approach. Future research can help to address additional areas, such as longitudinal research on discrimination and coping, and studies that advance the measurement of intersectional forms of minority stress.
References
Anderssen, Norman, Børge Sivertsen, Kari Jussie Lønning, and Kristi Malterud. 2020. “Life Satisfaction and Mental Health Among Transgender Students in Norway.” BMC Public Health 20 (1): Article 1.
Bowleg, Lisa. 2013. “‘Once You’ve Blended the Cake, You Can’t Take the Parts Back to the Main Ingredients’: Black Gay and Bisexual Men’s Descriptions and Experiences of Intersectionality.” Sex Roles 68 (11–12): 754–67.
Braksmajer, Amy, Janie Simmons, Angela Aidala, and James M. McMahon. 2018. “Effects of Discrimination on HIV-related Symptoms in Heterosexual Men of Color.” American Journal of Men’s Health 12 (6): 1855–63.
Brooks, Virginia R. 1981. Minority Stress and Lesbian Women. Lexington, MA: Lexington Books.
Budge, Stephanie L., Jill L. Adelson, and Kimberly A. S. Howard. 2013. “Anxiety and Depression in Transgender Individuals: The Roles of Transition Status, Loss, Social Support, and Coping.” Journal of Consulting and Clinical Psychology 81 (3): 545–57.
Carver, Charles S. 1997. “You Want to Measure Coping but Your Protocol’s Too Long: Consider the Brief Cope.” International Journal of Behavioral Medicine 4: 92–100.
Chan, Randolph C. H., Winnie W. S. Mak, Gloria Y. K. Ma, and Mandy Cheung. 2021. “Interpersonal and Intrapersonal Manifestations of HIV Stigma and Their Impacts on Psychological Distress and Life Satisfaction Among People Living with HIV: Toward a Dual-process Model.” Quality of Life Research 30 (1): 145–56.
Collins, Patricia H. 1990. Black Feminist Thought: Knowledge, Consciousness, and the Politics of Empowerment. London: Unwin Hyman.
Conlin, Sarah E., Richard P. Douglass, and Staci Ouch. 2019. “Discrimination, Subjective Wellbeing, and the Role of Gender: A Mediation Model of LGB Minority Stress.” Journal of Homosexuality 66 (2): 238–59.
Cuádraz, Gloria Holguín, and Lynet Uttal. 1999. “Intersectionality and In-depth Interviews: Methodological Strategies for Analyzing Race, Class, and Gender.” Race, Gender & Class 6 (3): 156–86.
Diener, Ed, Robert A. Emmons, Randy J. Larsen, and Sharon Griffin. 1985. “The Satisfaction with Life Scale.” Journal of Personality Assessment 49: 71–75.
DuBois, L. Zachary, Jae A. Puckett, Dee Jolly, Sally Powers, Tian Walker, Debra A. Hope, Richard Mocarski, T. Zachary Huit, Brenna R. Lash, Natalie Holt, Allura Ralston, Makinna Miles, A. Capannola, Clove Tipton, Geeta Eick, and Robert-Paul Juster. 2024. “Gender Minority Stress and Diurnal Cortisol Profiles Among Transgender and Gender Diverse People in the United States.” Hormones and Behavior 159: 105473.
Fergusson, David M., Geraldine McLeod, L. J. Horwood, Nicola R. Swain, Simone Chapple, and R. Poulton. 2015. “Life Satisfaction and Mental Health Problems (18 to 35 Years).” Psychological Medicine 45 (11): 2427–36.
Freese, Rebecca, Miles Q. Ott, Brian A. Rood, Sari L. Reisner, and David W. Pantalone. 2018. “Distinct Coping Profiles Are Associated with Mental Health Differences in Transgender and Gender Nonconforming Adults.” Journal of Clinical Psychology 74 (1): 136–46.
Grossman, Arnold H., Anthony R. D’Augelli, and John A. Frank. 2011. “Aspects of Psychological Resilience Among Transgender Youth.” Journal of LGBT Youth 8 (2): 103–15.
Grupp, Katharina, Marco Blessmann, Hans-Helmut König, and André Hajek. 2023. “Are Transgender People Satisfied with Their Lives?” BMC Public Health 23 (1): 1002.
Handal, Alexis J., Cirila Estela Vasquez Guzman, Alexandra Hernandez-Vallant, Alejandra Lemus, Julia Meredith Hess, Norma Casas, Margarita Galvis, Dulce Medina, Kimberly Huyser, and Jessica R. Goodkind. 2023. “Measuring Latinx/@ Immigrant Experiences and Mental Health: Adaptation of Discrimination and Historical Loss Scales.” American Journal of Orthopsychiatry 93 (1): 27–40.
Hayes, Andrew F. 2022. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-based Approach. 3rd ed. New York: The Guilford Press.
Hendricks, Michael L., and Ryan J. Testa. 2012. “A Conceptual Framework for Clinical Work with Transgender and Gender Nonconforming Clients: An Adaptation of the Minority Stress Model.” Professional Psychology: Research and Practice 43: 460–67.
Huynh, Kiet Duc, Nat L. Bricker, Debbiesiu L. Lee, and Kimberly F. Balsam. 2024. “Development and Validation of the LGBTQ2+ POC Microaggressions Scale—brief (LGBTQ2+ PCMS-B).” Stigma and Health 9 (3): 389–99.
James, Sandy E., Jody L. Herman, Susan Rankin, Mara Keisling, Lisa Mottet, and Ma’ayan Anafi. 2016. The Report of the 2015 US Transgender Survey. Washington, DC: National Center for Transgender Equality.
Janssen, Tim, Kristi E. Gamarel, Ethan H. Mereish, Suzanne M. Colby, Michelle Haikalis, and Kristina M. Jackson. 2023. “Associations Among Enacted Stigma, Perceived Chances for Success, Life Satisfaction, and Substance Use Among Sexual Minority and Heterosexual Youth.” Substance Use & Misuse 58 (9): 1121–31.
Kim, Eric S., Scott W. Delaney, Louis Tay, Ying Chen, Ed Diener, and Tyler J. VanderWeele. 2021. “Life Satisfaction and Subsequent Physical, Behavioral, and Psychosocial Health in Older Adults.” The Milbank Quarterly 99 (1): 209–39.
Krell, Elías Cosenza. 2017. “Is Transmisogyny Killing Trans Women of Color? Black Trans Feminisms and the Exigencies of White Femininity.” TSQ: Transgender Studies Quarterly 4 (2): 226–242.
Lawrence, Jourdyn A., Ichiro Kawachi, Kelle White, Mary T. Bassett, Naomi Priest, Joan Gakii Masunga, Hannah J. Cory, Carol Mita, and David R. Williams. 2022. “A Systematic Review and Meta-analysis of the Everyday Discrimination Scale and Biomarker Outcomes.” Psychoneuroendocrinology 142: 105772.
Lefevor, G. Tyler, Caroline C. Boyd-Rogers, Brianna M. Sprague, and Rebecca A. Janis. 2019a. “Health Disparities Between Genderqueer, Transgender, and Cisgender Individuals: An Extension of Minority Stress Theory.” Journal of Counseling Psychology 66 (4): 385–95.
Lefevor, G. Tyler, Rebecca A. Janis, Alexis Franklin, and William-Michael Stone. 2019b. “Distress and Therapeutic Outcomes Among Transgender and Gender Nonconforming People of Color.” The Counseling Psychologist 47 (1): 34–58.
Lindley, Louis, and Stephanie L. Budge. 2024. “Development and Validation of the Trans and Nonbinary Coping Measure (TNCM): A Measure of Trans and Nonbinary Specific Ways of Coping with Gender-related Stress.” Psychology of Sexual Orientation and Gender Diversity 11 (3): 425–41.
Meyer, Ilan H. 2003. “Prejudice, Social Stress, and Mental Health in Lesbian, Gay, and Bisexual Populations: Conceptual Issues and Research Evidence.” Psychological Bulletin 129 (5): 674–97.
Owens, Trenton K., Lauren Mizock, Alayne J. Ormerod, Annabelle Nelson, Colt St. Amand, Diane Paces-Wiles, and Terrence D. Judd. 2023. “‘Invisible in the Most Tragic of Ways’: Exploring Internalized Transphobia and Coping Through Photovoice.” Health Promotion Practice 24 (4): 682–93.
Phillips, Nia L., Glenn Adams, and Phia S. Salter. 2015. “Beyond Adaptation: Decolonizing Approaches to Coping with Oppression.” Journal of Social and Political Psychology 3 (1): 365–87.
Puckett, Jae A., Meredith R. Maroney, Lauren P. Wadsworth, Brian Mustanski, and Michael E. Newcomb. 2020. “Coping with Discrimination: The Insidious Effects of Gender Minority Stigma on Depression and Anxiety in Transgender Individuals.” Journal of Clinical Psychology 76 (1): 176–94.
Puckett, Jae A., Emmie Matsuno, Christina Dyar, Brian Mustanski, and Michael E. Newcomb. 2019. “Mental Health and Resilience in Transgender Individuals: What Type of Support Makes a Difference?” Journal of Family Psychology 33 (8): 954–64.
Reisner, Sari L., Jaclyn M. White, Judith B. Bradford, and Matthew J. Mimiaga. 2014. “Transgender Health Disparities: Comparing Full Cohort and Nested Matched-pair Study Designs in a Community Health Center.” LGBT Health 1 (3): 177–84. https://doi.org/10.1089/lgbt.2014.0009.
Rotondi, Nooshin Khobzi, Greta R. Bauer, Robb Travers, Anna Travers, Kyle Scanlon, and Matthias Kaay. 2011. “Depression in Male-to-Female Transgender Ontarians: Results From the Trans Pulse Project.” Canadian Journal of Community Mental Health 30 (2): 113–33.
Scheim, Ayden I., and Greta R. Bauer. 2019. “The Intersectional Discrimination Index: Development and Validation of Measures of Self-reported Enacted and Anticipated Discrimination for Intercategorical Analysis.” Social Science & Medicine 226: 225–35.
Sherman, Athena D. F., Monique Balthazar, Meredith Klepper, Sarah Febres-Cordero, Akshara Valmeekanathan, Dianne Prakash, Andrea N. Cimino, Whitney Wharton, Kisha Allure, and Ursula Kelly. 2022. “Approach and Avoidant Coping Among Black Transgender Women Who Have Experienced Violence: A Qualitative Analysis.” Psychological Services 19 (Suppl 1): 45–61.
Stotzer, Rebecca L. 2009. “Violence Against Transgender People: A Review of United States Data.” Aggression and Violent Behavior 14 (3): 170–79.
Taylor, Keeanga-Yamahtta, ed. 2017. How We Get Free: Black Feminism and the Combahee River Collective. Chicago: Haymarket Books.
Testa, Ryan J., Janice Habarth, Jayme Peta, Kimberly Balsam, and Walter Bockting. 2015. “Development of the Gender Minority Stress and Resilience Measure.” Psychology of Sexual Orientation and Gender Diversity 2 (1): 65–77.
Testa, Ryan J., Matthew S. Michaels, Whitney Bliss, Megan L. Rogers, Kimberly F. Balsam, and Thomas Joiner. 2017. “Suicidal Ideation in Transgender People: Gender Minority Stress and Interpersonal Theory Factors.” Journal of Abnormal Psychology 126: 125–36.
Tompkins, Avery Brooks. 2021. “Transgender as a Term.” In The SAGE Encyclopedia of Trans Studies, edited by Abbie E. Goldberg and Genny Beemyn, 859–62. Thousand Oaks, CA: Sage.
Vargas, Sylvanna M., Stanley J. Huey, and Jeanne Miranda. 2020. “A Critical Review of Current Evidence on Multiple Types of Discrimination and Mental Health.” American Journal of Orthopsychiatry 90 (3): 374–90.
Whitaker, Kara M., Susan A. Everson-Rose, James S. Pankow, Carlos J. Rodriguez, Tené T. Lewis, Kiarri N. Kershaw, Ana V. Diez Roux, and Pamela L. Lutsey. 2017. “Experiences of Discrimination and Incident Type 2 Diabetes Mellitus: The Multi-ethnic Study of Atherosclerosis (MESA).” American Journal of Epidemiology 186 (4): 445–55.
Williams, David R., Hector M. González, Stacey Williams, Selina A. Mohammed, Hashim Moomal, and Dan J. Stein. 2008. “Perceived Discrimination, Race and Health in South Africa: Findings from the South Africa Stress and Health Study.” Social Science and Medicine 67 (3): 441–52.
Williams, David R., Yan Yu, James S. Jackson, and Norman B. Anderson. 1997. “Racial Differences in Physical and Mental Health: Socio-economic Status, Stress and Discrimination.” Journal of Health Psychology 2 (3): 335–51.
Zilioli, Samuele, Yanping Jiang, DeAnnah Byrd, and Nataria Joseph. 2023. “Lifetime Discrimination, Habitual and Daily Everyday Discrimination, and Diurnal Cortisol Among Older African American Adults.” Psychoneuroendocrinology 152: 106089.
| Demographic Variable | n | % |
|---|---|---|
| Gender | ||
| Trans man | 37 | 23.4% |
| Trans woman | 32 | 20.3% |
| Genderqueer | 16 | 10.1% |
| Nonbinary | 40 | 25.3% |
| Agender | 3 | 1.9% |
| Androgyne | 1 | 0.6% |
| Genderfluid | 2 | 1.3% |
| Woman | 9 | 5.7% |
| Man | 6 | 3.8% |
| Bigender | 2 | 1.3% |
| Not listed | 9 | 5.7% |
| Missing | 1 | 0.6% |
| Sex Assigned at Birth | ||
| Male | 52 | 33.1% |
| Female | 106 | 66.9% |
| Race/Ethnicity | ||
| Black or African American | 8 | 5.1% |
| American Indian or Alaskan Native | 2 | 1.3% |
| Asian | 6 | 3.8% |
| Latinx | 6 | 3.8% |
| White | 109 | 69.0% |
| Not listed | 1 | 0.6% |
| Multiracial/ Multiethnic | 26 | 16.5% |
| State | ||
| Oregon | 45 | 28.5% |
| Michigan | 39 | 24.7% |
| Nebraska | 35 | 22.2% |
| Tennessee | 39 | 24.7% |
| Location Type | ||
| Urban | 76 | 48.1% |
| Suburban | 55 | 35.1% |
| Rural | 27 | 16.9% |
| Income | ||
| Less than $10,000 | 43 | 27.4% |
| $10,000 – $19,999 | 38 | 24.2% |
| $20,000 – $29,999 | 16 | 10.1% |
| $30,000 – $39,999 | 12 | 7.6% |
| $40,000 – $49,999 | 11 | 7.0% |
| $50,000 – $59,999 | 14 | 8.9% |
| $60,000 – $69,999 | 5 | 3.2% |
| $70,000 – $79,999 | 8 | 5.1% |
| $80,000 – $89,999 | 4 | 2.5% |
| $90,000 or more | 6 | 3.8% |
| Education Level | ||
| High school graduate – high school diploma or equivalent (i.e. GED) | 14 | 8.9% |
| Some college credit, but less than 1 year | 8 | 5.1% |
| Technical or vocational school degree | 5 | 3.2% |
| One or more years of college, no degree | 42 | 26.6% |
| Associate’s degree | 18 | 11.4% |
| Bachelor’s degree | 52 | 32.9% |
| Master’s degree | 16 | 10.1% |
| Doctorate or professional degree | 2 | 1.3% |
| Graduate of a Certificate Program | 1 | 0.6% |
| Number of Discrimination Experiences | n | Percent of Sample |
| 0 | 56 | 35.89% |
| 1 | 24 | 15.38% |
| 2 | 29 | 18.58% |
| 3 | 18 | 11.54% |
| 4 | 11 | 7.05% |
| 5 | 8 | 5.13% |
| 6 | 6 | 3.85% |
| 7 | 3 | 1.92% |
| 8 | 1 | 0.64% |
Note. Two participants were missing data on this questionnaire. Percentages were calculated based on 156 participants who completed this questionnaire.
| Discrimination Variable | n (%) |
| At any time in your life, have you ever been unfairly fired? | 44 (28.21%) |
|
Most common identity endorsed: gender expression or presentation |
26 (59.09% of participants who endorsed this form of discrimination) |
| For unfair reasons, have you ever not been hired for a job? | 46 (29.49%) |
|
Most common identity endorsed: gender expression or presentation |
33 (71.74% of participants who endorsed this form of discrimination) |
| Have you ever been unfairly denied a promotion? | 40 (25.64%) |
|
Most common identity endorsed: gender identity |
25 (62.50% of participants who endorsed this form of discrimination) |
| Have you ever been unfairly stopped, searched, or questions, physically threatened or abused by the police? | 39 (25.00%) |
|
Most common identity endorsed: gender expression or presentation |
23 (58.97% of participants who endorsed this form of discrimination) |
| Have you ever been unfairly discouraged by a teacher or advisor from continuing your education? | 29 (18.59%) |
|
Most common identity endorsed: gender expression or presentation |
17 (58.62% of participants who endorsed this form of discrimination) |
| Have you ever been unfairly prevented from moving into a neighborhood because the landlord or a realtor refused to sell or rent you a house or apartment? | 14 (8.97%) |
|
Most common identity endorsed: race; sexual orientation (equal endorsement) |
7 (50.00% of participants who endorsed this form of discrimination) |
| Have you ever moved into a neighborhood where neighbors made life difficult for you or your family? | 28 (17.95%) |
|
Most common identity endorsed: gender expression or presentation |
20 (71.42% of participants who endorsed this form of discrimination) |
| Have you ever been unfairly denied a bank loan? | 2 (1.28%) |
|
Most common identity endorsed: gender identity; age (equal endorsement) |
1 (50.00% of participants who endorsed this form of discrimination) |
| Have you ever received service from someone such as a plumber or car mechanic that was worse than what other people get? | 43 (27.56%) |
|
Most common identity endorsed: gender expression or presentation |
35 (81.39% of participants who endorsed this form of discrimination) |
Note. Two participants were missing data on this questionnaire. Percentages were calculated based on 156 participants who completed this questionnaire. We caution against use of percentages for some responses as the sample size for select questions was very small (e.g., denial of a bank loan).
| Satisfaction with Life | |||
| Variable | b | SE | R2 |
| Lifetime Discrimination | 1.44 | 1.02 | 0.23** |
| Cluster 1: Functional Coping | 7.02** | 1.71 | |
| Cluster 3: Undifferentiated Coping | 6.87** | 1.76 | |
| Discrimination X Cluster 1 | –2.41* | 1.12 | 𝛥R2 = 0.04* |
| Discrimination X Cluster 3 | –3.20** | 1.13 | |
Note. Reference group = Cluster 2: Unhelpful Coping; Analysis controlled for age; * p < .05, ** p < .01
| Satisfaction with Life | |||
| Variable | b | SE | R2 |
| Enacted Stigma | 0.32 | 0.77 | 0.19** |
| Cluster 1: Functional Coping | 7.78** | 1.99 | |
| Cluster 3: Undifferentiated Coping | 7.72** | 2.03 | |
| Enacted Stigma X Cluster 1 | –1.03 | 0.81 | 𝛥R2 = 0.01 |
| Enacted Stigma X Cluster 3 | –0.93 | 0.84 | |
Note. Reference group = Cluster 2: Unhelpful Coping; Analysis controlled for age; * p < .05, ** p < .01